Login
Registration enables users to use special features of this website, such as past
order histories, retained contact details for faster checkout, review submissions, and special promotions.
order histories, retained contact details for faster checkout, review submissions, and special promotions.
Forgot password?
Registration enables users to use special features of this website, such as past
order histories, retained contact details for faster checkout, review submissions, and special promotions.
order histories, retained contact details for faster checkout, review submissions, and special promotions.
Quick Order
Products
Antibodies
ELISA and Assay Kits
Research Areas
Infectious Disease
Resources
Purchasing
Reference Material
Contact Us
Location
Corporate Headquarters
Vector Laboratories, Inc.
6737 Mowry Ave
Newark, CA 94560
United States
Telephone Numbers
Customer Service: (800) 227-6666 / (650) 697-3600
Contact Us
Additional Contact Details
Login
Registration enables users to use special features of this website, such as past
order histories, retained contact details for faster checkout, review submissions, and special promotions.
order histories, retained contact details for faster checkout, review submissions, and special promotions.
Forgot password?
Registration enables users to use special features of this website, such as past
order histories, retained contact details for faster checkout, review submissions, and special promotions.
order histories, retained contact details for faster checkout, review submissions, and special promotions.
Quick Order
| Catalog Number | Size | Price |
|---|---|---|
| LS-C132023-2 | 2 ml | $553 |
Polyclonal Human anti‑Human TOP1 / Topoisomerase I Antibody LS‑C132023
Polyclonal Human anti‑Human TOP1 / Topoisomerase I Antibody LS‑C132023
Antibody:
TOP1 / Topoisomerase I Human anti-Human Polyclonal Antibody
Application:
ELISA, ID
Reactivity:
Human
Format:
Unconjugated, Unmodified
Toll Free North America
 (800) 227-6666
(800) 227-6666
For Research Use Only
Overview
Antibody:
TOP1 / Topoisomerase I Human anti-Human Polyclonal Antibody
Application:
ELISA, ID
Reactivity:
Human
Format:
Unconjugated, Unmodified
Specifications
Description
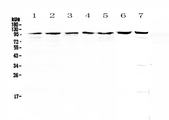
Topoisomerase I antibody LS-C132023 is an unconjugated human polyclonal antibody to human Topoisomerase I (TOP1). Validated for ELISA and ID.
Target
Human TOP1 / Topoisomerase I
Synonyms
TOP1 | DNA topoisomerase I | DNA topoisomerase 1 | TOPI | Topoisomerase (DNA) I | Topoisomerase I | Type I DNA topoisomerase
Host
Human
Reactivity
Human
(tested or 100% immunogen sequence identity)
Clonality
Polyclonal
Conjugations
Unconjugated
Purification
Delipidated and defibrinated
Modifications
Unmodified
Immunogen
Human Scl-70 Antigen from human plasma.
Specificity
Recognizes human Scl-70 antigen. Does not recognize purified SSA, SSB, Sm, Sm/RNp and Jo-1 antigen.
Applications
- ELISA
- Immunodiffusion
Usage
Suitable for use in DNA conformational analysis and topology as well as DNA repair, drug resistance, cell proliferation and leukemia studies. The double-helical configuration that DNA strands naturally reside in makes them difficult to separate, and yet they must be separated if enzymes are to transcribe the sequences that encode proteins, or if chromosomes are to be replicated. In so-called circular DNA, in which double helical segment is bent around and joined in a circle, the two strands are topologically linked, or knotted. They cannot be separated by any process that does not involve the breaking of strands. Topoisomerases catalyze and guide the unknotting of DNA. Type I topoisomerases cut only one strand of DNA; type I topoisomerase of E. coli > E. coli (omega protein) relaxes negatively supercoiled DNA and does not act on positively supercoiled DNA. Type II topoisomerases cut both strands of DNA; type II topoisomerase of E. coli (DNA gyrase) increases the degree of negative supercoiling in DNA and requires ATP. It is inhibited by several antibiotics, including nalidixic acid and ovobiocin. Antibodies generated against the nuclear constituents are known as antinuclear antibodies (ANA). This includes autoantibodies directed against the extractable (soluble in physiological buffers) nuclear antigen or ENA. The most prominent of ANAs/ENAs are autoantibodies which binds to ds-DNA, ss-DNA, histones, ribonucleoproteins (RNP) and the SS-A, SS-B, Sm antigens, Jo-1, and Scl-70. Two antibodies, anti-dsDNA and anti-Sm, appear to occur only in SLE. Others occur in a variety of autoimmune and mixed connective tissue diseases. Antibody to Scl-70 antigen was originally called Scl-1. Anti-Scl-70 has been shown to react with a cellular antigen known as DNA topoisomerase I, which is responsible for the relaxation of supercoiled DNA. Anti-Scl-70 is found in ~75% patients with the diffuse progressive form of scleroderma. The presence of anti-Scl-70 seems to exclude the presence of anti-centromere antibody, which is a marker for a subset of patients with scleroderma known as CREST (calcinosis, sclerodactyly, and telangiectasia) syndrome. The frequency of ANA-positives in various rheumatic diseases has been reported for SLE, rheumatoid arthritis (RA), progressive systemic sclerosis (PSS), polymyositis (PM), dermatomyositis (DM), mixed connective tissue diseases, drug-induced SLE, and Sjogren's syndrome (SS). Most of these studies are based on tedious fluorescent ANA (FANA). Other techniques such as RIA, immunodiffusion, hemagglutination, electrophoresis and immunoblotting are also used to define antibody specificity. Recently, immunological assays (mostly ELISA) that determine the specificity of ANA have been used in studying patients with systemic rheumatic diseases. Applications. Suitable for use in ELISA and Immunodiffusion.
Presentation
Lyophilized from PBS, pH 7.2, 0.02% Sodium Azide
Reconstitution
Reconstitute with 2 ml of sterile distilled water.
Storage
Lyophilized powder may be stored at -20°C. Stable for 1 year at -20°C. Aliquot to avoid freeze-thaw cycles. Store at -20°C. Reconstituted product is stable for 1 year at -20°C.
Restrictions
For research use only. Intended for use by laboratory professionals.
About TOP1 / Topoisomerase I
Publications (0)
Customer Reviews (0)
Featured Products

Species:
Human, Mouse
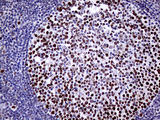
Applications:
IHC, IHC - Paraffin, Western blot, Immunoprecipitation
Species:
Human, Mouse
Applications:
IHC, Western blot, Immunoprecipitation, ELISA
Species:
Human
Applications:
IHC, Western blot

Reactivity:
Human
Range:
0.156-10 ng/ml
Request SDS/MSDS
To request an SDS/MSDS form for this product, please contact our Technical Support department at:
Technical.Support@LSBio.com
Requested From: United States
Date Requested: 4/3/2025
Date Requested: 4/3/2025



